
It’s a statistic you’ve probably seen before. Individuals with serious mental illness die, on average, 15 to 30 years younger than those individuals without. What you may not know is that this difference represents the largest health disparity in the US. It’s larger than the gender, racial and socioeconomic gap in mortality. And unlike some of the other gaps that have begun to slowly close over the years, this gap isn’t shrinking.
For individuals with serious mental illness, it is easy to assume that their high mortality rate is due to some sequela of their mental illness—suicide, overdose, accident. But this is simply not the case. Individuals with serious mental illnesses are overwhelmingly dying not from their mental health conditions but instead from the same physical health conditions plaguing the general public—cancer, heart disease, diabetes,.
What’s Causing the Disproportionately High Mortality Rate?
Like most questions related to health, the answer involves a complex interplay of many factors.
- Risk Factors: Individuals with serious mental illness are more likely to have or engage in risky health behaviors, for example they are more than twice as likely to use tobacco
- High Rates of Comorbidity: All relationships may not be fully understood yet, but the data clearly shows high rates of comorbidity between serious mental illness and cardiovascular disease, diabetes and stroke.
- Health System Factors: Individuals with serious mental illness are less likely to receive primary care, and instead access the public mental health system and/or psychiatrists as their primary healthcare providers.
- Clinician Bias: Dhurv Khullar writes in the New York Times that there are likely two clinician biases at play as well.
- Therapeutic Pessimism. Khullar describes this as the belief some clinicians have that people with serious mental illness won’t get better. And this belief can lead to a “what’s the point” approach to treatment.
- Diagnostic Overshadowing. This refers to the bias towards attributing every patient complaint to their mental illness. This can lead to serious complaints or concerns not being followed up on. One study found that patients with mental illness were significantly less likely to undergo cardiac catheterization when they have heart attack symptoms and another study found individuals with mental illness were less likely to receive cancer screening and follow up care.
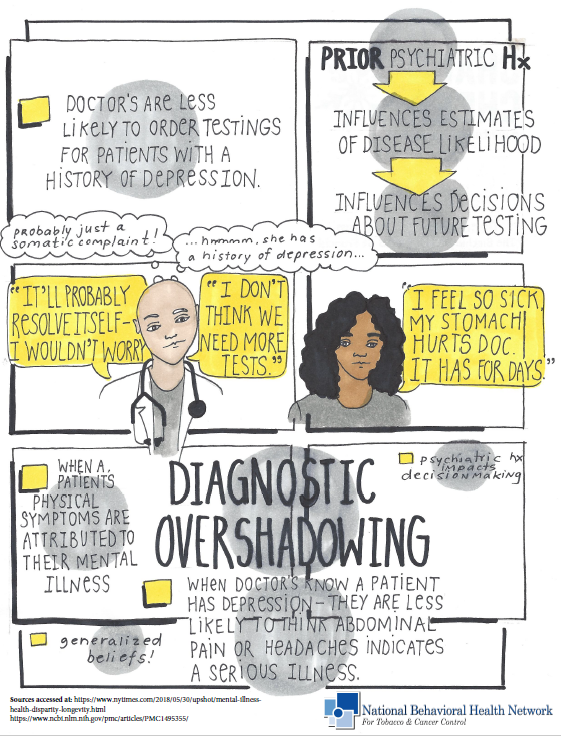
Click here to view an infographic about Diagnostic Overshadowing created by NBHN Director Taslim van Hattum.
From Dr. Lisa Rosenbaum, as quoted the New York Times: “Many of us have internalized the directive to seek a test or procedure only if ‘there’s something you can do about it.’ For mentally ill patients with medical illness, however, this principle often justifies doing nothing.”
What Can Be Done?
Unsurprisingly, the solution is multifaceted and still developing. Below are a few things that health professionals can do.
- Integrate Primary Health Care into Behavioral Health Care. In recent years there has been a push to integrate mental health care into primary care settings, but the integration can happen the other way too. If you work in a behavioral health setting, consider implementing cancer screenings, whole health programs, and/or tobacco cessation programming. For more information on any of the following, see below.
- Reverse Integration
- Cancer Programming.
- Webinar: Cancer Prevention Approaches for Individuals with Behavioral Health Conditions
- Webinar: Implementing Cancer Screenings Referrals Within Community Behavioral Health Organizations
- Webinar: Addressing Needs Across the Cancer Continuum for Individuals Behavioral Health Populations
- CDC Cancer Educational Campaigns
- Whole Health Programming.
- BHWP Well Body Program: https://www.bhwellness.org/programs/wellbody
- Tobacco Cessation Resources.
- Webinar: Smoking Cessation Intervention for Behavioral Health Populations
- Webinar: Use of Tips For Former Smokers Campaign In Clinical Settings
- Webinar: The Power of Peers for Tobacco and Cancer Control Practices
- Article: Helping Smokers Quit: New Partners and New Strategies from the University of California, San Francisco Smoking Cessation Leadership Center
- Blog Post: Igniting Motivation: Using Peers to Spark Your Tobacco Cessation Services
- UC’s Behavioral Health and Wellness’s Tobacco Free Program
- UCSF’s Smoking Cessation Leadership Center’s RX for Change Program
- Check Your Biases. This is without question a challenging undertaking, nonetheless, it is essential in the fight to close the disparities gap! If you are a clinician working with an individual diagnosed with a serious mental illness, here are some things you can ask yourself:
- Has this patient been screened for cancer? Diabetes? Heart Disease?
- Does this patient have modifiable risky health behaviors such as tobacco utilization? If so, have you begun to engage in conversations with the patient about quitting smoking? If not, why?
- Does your treatment plan for your patients with serious mental illness include plans to address their physical health in addition to their mental health? If not, why?
- Has your patient complained about health concerns during recent visits? If so, have these been followed up on? If not, why?
For more information on how to reduce implicit clinician bias, take a look at this article from the Institute for Healthcare Improvement.